AV Node Ablation
AV Node Ablation
What is AV node ablation?
How the heart's electrical system works
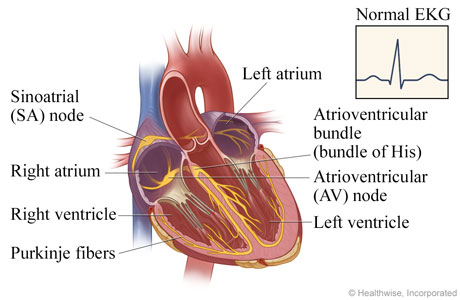
In a normal heart, electrical impulses pace the rhythm at which the heart contracts and relaxes. The sinoatrial (SA) node triggers the electrical impulse, causing the upper chambers (atria) to contract. The signal travels through the atrioventricular (AV) node to the atrioventricular bundle, which divides into the Purkinje fibers that carry the signal and cause the lower chambers (ventricles) to contract. The electrocardiogram (EKG, ECG) shows this normal electrical activity.
How atrial fibrillation happens
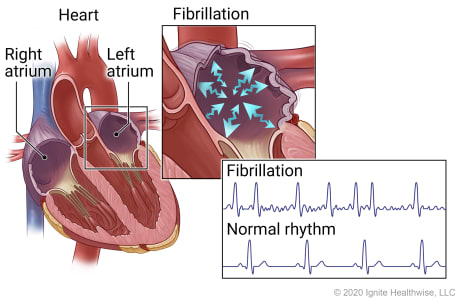
In atrial fibrillation, erratic electrical impulses in the upper chambers of the heart (atria) cause those chambers to fibrillate, or quiver. This results in an irregular and frequently rapid heart rate. The irregular, sawtooth pattern in the electrocardiogram (EKG, ECG) shows these erratic impulses.
Catheter is threaded through a vein to the heart
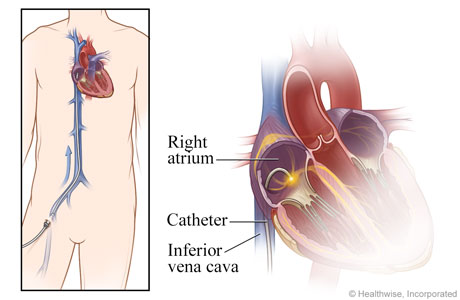
For this nonsurgical procedure, catheters are inserted into a vein, typically in the groin or neck, and threaded through the vena cava vein into the right atrium of the heart.
AV node is destroyed
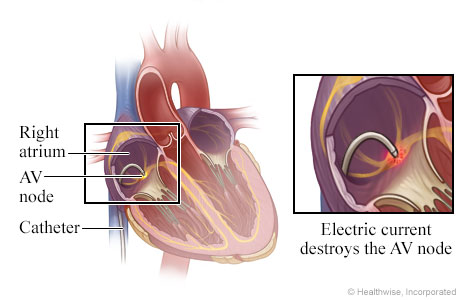
An electrode at the tip of the catheter sends out energy, such as radio waves, that destroys (ablates) the atrioventricular (AV) node or other heart tissue that is responsible for the erratic impulses.
Pacemaker controls the heart rhythm
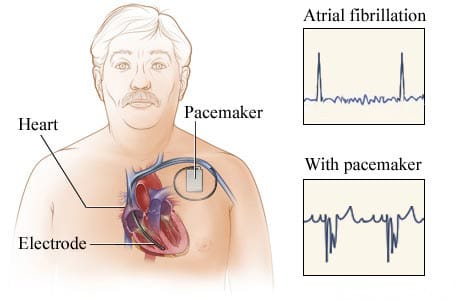
When the AV node is ablated, a permanent pacemaker is implanted that paces the ventricle. The pulse generator and battery part of the pacemaker are implanted under the skin of the chest. The electrocardiograms (EKG, ECG) show the heart's electrical activity during atrial fibrillation and when a heart has a pacemaker.
Appointment Information
Call us at 888-287-1082 to schedule an appointment with a U-M Cardiovascular Center physician, get a prescription refill, or request to speak with your nurse. Or visit the Make a Cardiovascular Appointment page to learn what to expect when you call us.
How is the procedure performed?
During the procedure, a catheter is inserted into a vein in the area of the groin and guided up to the AV node. Radiofrequency energy is passed through the catheter to destroy the node. This eliminates the rapid and irregular heartbeats caused by atrial fibrillation.
Because the pulse rate typically drops to a very slow rate as a result of the procedure, a pacemaker is implanted to increase the heart rate at rest and during exertion or exercise, simulating a normal heart rhythm.
The pacemaker is an electronic device made up of a pulse generator and leads (wires). The device is implanted in the upper chest, under the skin. It is connected to one or two leads that are inserted through a vein into the heart, delivering painless electric pulses that stimulate the heart to beat faster when necessary.
The AV node ablation procedure (including implantation of a pacemaker) takes about three hours to perform and the patient typically spends two nights in the hospital before going home.
What are the advantages of AV node ablation?
AV node ablation with pacemaker implantation has a very high success rate and low risk of serious complications while being effective in alleviating symptoms caused by a rapid and/or irregular heart rate. The procedure also eliminates the need for medications aimed at preventing atrial fibrillation and controlling heart rate.
Because AV node ablation does not cure atrial fibrillation, the patient is dependent on a pacemaker for the rest of his or her life and will have to continue taking a blood thinner to prevent strokes.
What are the risk factors of AV node ablation?
There is a 1 or 2 percent risk of a complication during the pacemaker implantation procedure, including:
- Infection
- Puncture of a lung
- Displacement of one of the pacemaker wires, which requires another procedure to reposition the wire in the heart
Locations
-
Electrophysiology Services | Cardiovascular Center 1425 E Ann St
Floor 3 Reception C
Ann Arbor, MI 48109-5856Get Directions
Doctors
Kelly Arps, MD
Clinical Assistant Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease

Apurba Kent Chakrabarti, MD
Clinical Assistant Professor
Cardiovascular Disease, Internal Medicine
Aman Chugh, MD
Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease

Thomas Christopher Crawford, MD
Clinical Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease
Amrish Deshmukh, MD
Clinical Assistant Professor
Cardiac Electrophysiology, Cardiovascular Disease, Internal Medicine

Hamid Ghanbari, MD
Clinical Associate Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease
Michael Ghannam, MD
Clinical Assistant Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease

Emma Hegwood, DO
Clinical Assistant Professor
Cardiac Electrophysiology, Cardiovascular Disease, Internal Medicine

Krit Jongnarangsin, MD
Clinical Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease

Rakesh Latchamsetty, MD
Clinical Associate Professor
Cardiac Electrophysiology, Internal Medicine, Cardiovascular Disease




News & Stories

Treating a rare coronary artery aneurysm without open heart surgery

A heart attack 9 days after giving birth: Mother of 4 shares her SCAD experience
A night of two national titles for U-M, as scientists and basketball players both triumph

Failed TAVR? Heart surgeons explain TAVR explant, options and risks

Six U-M medical research teams picked for virtual science tournament