
Introduction
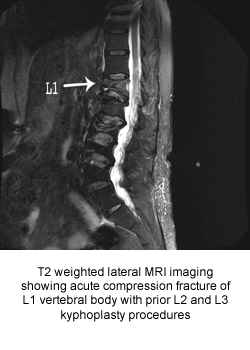
A compression fracture is a type of fracture in which the vertebral body collapses more in the front producing a wedge shaped vertebrae. This can be caused by osteoporosis or cancer involving the vertebral body.
Risk factors
Osteoporosis
Osteoporosis is a disease that thins and weakens the bones to the point that they become fragile and break easily. Women and men with osteoporosis most often break bones in the hip, spine, and wrist. There are several causes and types of osteoporosis. The first is primary osteoporosis, which has two types - (I) and (II).
Type I is an excessive loss of the spongy tissue of the bone (cancellous bone), with some sparing of outer bone. This type of osteoporosis is six times more common in women than men, and the onset usually occurs in the 15-20 years following menopause. The loss of bone is thought to be linked to an estrogen deficiency in women and a testosterone deficiency in men — both of which are due to aging. In this type of osteoporosis, vertebral spine fractures are the most common result.
Type II refers to a simultaneous loss of both the outer bone and the spongy tissue inside the bone. This type is only two times more common in women than men. It typically occurs once people reach their 70s and 80s. It is also thought to be the result of a deficiency in dietary calcium, age-related Vitamin D decline, or increased activity of the parathyroid glands (secondary hyperparathyroidism). Hip fractures are the most common result of this type of osteoporosis.
Secondary osteoporosis, also known as "high-turnover osteoporosis," is a condition of an increased rate of bone remodeling — or an increase in the amount of bone being remodeled. This condition causes an overall increase in the rate of bone loss. Bone turnover is caused by two functions: (1) the production of new bone, and (2) the loss (resorption) of old bone. The amount of bone mass you have depends on the balance between these functions, which is your bone turnover rate. If you have a high turnover rate, you are at greater risk for developing osteoporosis. Secondary osteoporosis can also have four hormonal causes:
- Hyperparathyroidism – increased activity of the parathyroid glands
- Hyperthyroidism – an excessive secretion of the thyroid glands
- Diabetes – a disease where the body does not produce or use insulin correctly (This leads to: hyperglycemia — an increase in blood sugar, increasing susceptibility to infection, and glycosuria — glucose in the urine)
- Hypercortisolism – a result of systemic illness or long-term use of oral corticosteroid
Osteoporosis can also be the result of disorders where the bone marrow cavity expands at the expense of the trabecular bone. The trabecular bones have a honeycomb appearance and large marrow spaces. They are called cancellous or spongious bone, and are found along lines of stress created by weight-bearing forces. If a trabecular bone is affected by increased bone marrow cavities, it loses some of its strength.
Other links to secondary osteoporosis are:
- Thalassemia - a hereditary form of anemia
- Multiple myeloma - multiple tumors within the bone and bone marrow
- Leukemia - a serious disease that is characterized by unrestrained growth of white blood cells in the tissues
- Metastatic bone diseases - when malignant tumor cells spread from one part of the body to another; the disease travels through the blood and settles in the bones
Cancer involving the vertebral body is common in patients diagnosed late in the course of their disease. The resulting change in height and spinal alignment can lead to serious health problems, including:
- chronic or severe pain
- limited function and reduced mobility
- loss of independence in daily activities
- decreased lung capacity
- difficulty sleeping
The first osteoporotic fracture makes it five times more likely further fractures will occur.
Treatment
Acute compression fractures are usually managed with 3 months of spinal bracing with a thoracolumbosacral orthosis (TLSO), also called an underarm or low-profile brace, and narcotics to stabilize the fracture and reduce pain. Vertebroplasty and kyphoplasty are both minimally-invasive surgical procedures for treating osteoporotic fractures where an orthopedic cement is injected directly into the fractured bone. This stabilizes the fracture. Patients are also prescribed oral medications for osteoporosis to prevent further bone loss.
Vertebroplasty
A hollow needle (trocar) is passed into the vertebral bone and a cement mixture including polymethylmethacrylate (PMMA), barium powder and a solvent is injected. The cement mixture resembles toothpaste or epoxy. The physician will monitor the entire procedure on a fluoroscopy imaging screen and make sure that the cement mixture does not back up into the spinal canal. Sedation medication will be administered through an intravenous catheter. A Foley catheter may be placed in your bladder. You will be attached to equipment that monitors your heart beat and blood pressure throughout the procedure.
Kyphoplasty
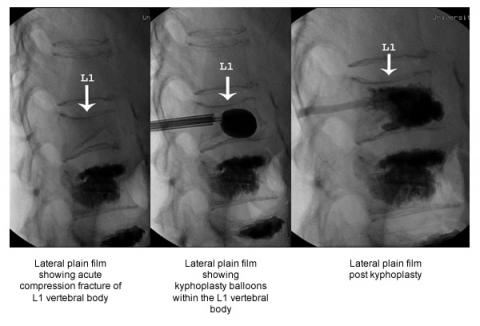
Kyphoplasty is similar to vertebroplasty except it includes an additional step. Prior to injecting the cement mixture, a special balloon is inserted and gently inflated inside the fracture vertebrae. The goal of this step is to restore height to the bone thus reducing the deformity of the spine. Most patients return to their normal daily activities one to two days after either procedure.
Limitations of Vertebroplasty/Kyphoplasty (V/K)
- V/K is not used for herniated disks or arthritic back pain.
- V/K is not generally recommended for otherwise healthy younger patients, mostly because there is limited experience with cement in the vertebral body for longer time periods.
- V/K cannot serve as a preventative treatment to help patients with osteoporosis avoid future fractures. It is used only to repair a known, non-healing fracture.
- V/K will not completely correct an osteoporosis-induced curvature of the spine, but it may keep the curve from getting worse.
- Patients with healed vertebral fractures are not candidates.
- It may be difficult for someone with severe emphysema or other lung diseases to lie flat for the one to two hours required to perform the procedure.