Childhood Non-Hodgkin Lymphoma Treatment (PDQ®): Treatment - Patient Information [NCI]
This information is produced and provided by the National Cancer Institute (NCI). The information in this topic may have changed since it was written. For the most current information, contact the National Cancer Institute via the Internet web site at http://cancer.gov or call 1-800-4-CANCER.
Childhood non-Hodgkin lymphoma is a disease in which malignant (cancer) cells form in the lymph system, which is a part of the body's immune system.
The immune system helps protect the body from infection and disease.
The lymph system is made up of the following:
- Lymph: Colorless, watery fluid that travels through the lymph vessels and carries lymphocytes (white blood cells).
- B lymphocytes, also called B cells, make antibodies to help fight infection. Most types of non-Hodgkin lymphoma begin in B lymphocytes.
- T lymphocytes, also called T cells, help B lymphocytes make the antibodies that help fight infection.
- Natural killer cells, also called NK cells, attack cancer cells and viruses.
- Lymph vessels: A network of thin tubes that collect lymph from different parts of the body and return it to the bloodstream.
- Lymph nodes: Small, bean-shaped structures that filter lymph and store white blood cells that help fight infection and disease. Lymph nodes are found along a network of lymph vessels throughout the body. Groups of lymph nodes are found in the neck, underarm, mediastinum (the area between the lungs), abdomen, pelvis, and groin.
- Spleen: An organ that makes lymphocytes, stores red blood cells and lymphocytes, filters the blood, and destroys old blood cells. The spleen is on the left side of the abdomen near the stomach.
- Thymus: An organ in which T lymphocytes mature and multiply. The thymus is in the chest behind the breastbone.
- Tonsils: Two small masses of lymph tissue at the back of the throat. There is one tonsil on each side of the throat.
- Bone marrow: The soft, spongy tissue in the center of certain bones, such as the hip bone and breastbone. White blood cells, red blood cells, and platelets are made in the bone marrow.
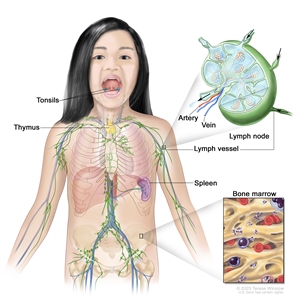
The lymph system is part of the body's immune system and is made up of tissues and organs that help protect the body from infection and disease. These include the tonsils, thymus, spleen, bone marrow, lymph vessels, and lymph nodes. Lymph (clear, watery fluid) and lymphocytes (white blood cells) travel through the lymph vessels and into the lymph nodes where the lymphocytes destroy harmful substances. The lymph enters the bloodstream through a large vein near the heart.
Lymph tissue is also found in other parts of the body such as the stomach, thyroid gland, brain, and skin.
Non-Hodgkin lymphoma can begin in B lymphocytes, T lymphocytes, or natural killer cells.
There are two general types of lymphomas: Hodgkin lymphoma and non-Hodgkin lymphoma. This summary is about the treatment of childhood non-Hodgkin lymphoma. For information about the treatment of childhood Hodgkin lymphoma, see Childhood Hodgkin Lymphoma Treatment.
Treatment of non-Hodgkin lymphoma is different for children and adults. For information about treatment of adults, see the following:
- Adult Non-Hodgkin Lymphoma
- Primary CNS Lymphoma Treatment
- Mycosis Fungoides (Including Sezary Syndrome) Treatment
There are three major types of childhood non-Hodgkin lymphoma.
The type of lymphoma is determined by how the cells look under a microscope. The three major types of childhood non-Hodgkin lymphoma are:
Aggressive mature B-cell non-Hodgkin lymphoma
Aggressive mature B-cell non-Hodgkin lymphomas include:
- Burkitt lymphoma/leukemia: Burkitt lymphoma and Burkitt leukemia are different forms of the same disease. Burkitt lymphoma/leukemia is an aggressive (fast-growing) disorder of B lymphocytes that is most common in children and young adults. It may form in the abdomen, Waldeyer's ring, testicles, bone, bone marrow, skin, central nervous system (CNS), or head and neck. Burkitt leukemia may start in the lymph nodes as Burkitt lymphoma and then spread to the blood and bone marrow, or it may start in the blood and bone marrow without forming in the lymph nodes first.
Both Burkitt leukemia and Burkitt lymphoma have been linked to infection with the Epstein-Barr virus (EBV), although EBV infection is more likely to occur in patients in Africa than in the United States. Burkitt lymphoma/leukemia is more common in White people. Burkitt lymphoma/leukemia is diagnosed when a sample of tissue is checked and a certain change to the MYCgene is found.
- Diffuse large B-cell lymphoma: Diffuse large B-cell lymphoma is the most common type of non-Hodgkin lymphoma. It is a type of B-cell non-Hodgkin lymphoma that grows quickly in the lymph nodes. The spleen, liver, bone marrow, or other organs are also often affected. Diffuse large B-cell lymphoma occurs more often in adolescents than in children.
- Primary mediastinal B-cell lymphoma: A type of lymphoma that develops from B cells in the mediastinum (the area between the lungs). It may spread to nearby organs including the lungs and the sac around the heart. It may also spread to lymph nodes and distant organs including the kidneys. Primary mediastinal B-cell lymphoma occurs more often in older adolescents than in children.
Lymphoblastic lymphoma
Lymphoblastic lymphoma is a type of lymphoma that mainly affects T-cell lymphocytes. It usually forms in the mediastinum (the area between the lungs). This causes trouble breathing, wheezing, trouble swallowing, or swelling of the head and neck. It may spread to lymph nodes, bone, bone marrow, skin, the CNS, abdominal organs, and other areas. Lymphoblastic lymphoma is a lot like acute lymphoblastic leukemia (ALL).
Anaplastic large cell lymphoma
Anaplastic large cell lymphoma is a type of lymphoma that mainly affects T-cell lymphocytes. It usually forms in the lymph nodes, skin, or bone, and sometimes forms in the gastrointestinal tract, lung, tissue that covers the lungs, and muscle. Patients with anaplastic large cell lymphoma have a receptor, called CD30, on the surface of their T cells. In many children, anaplastic large cell lymphoma is marked by changes in the ALK gene that makes a protein called anaplastic lymphoma kinase. A pathologist checks for these cell and gene changes to help diagnose anaplastic large cell lymphoma.
Some types of non-Hodgkin lymphoma are rare in children.
Some types of childhood non-Hodgkin lymphoma are less common. These include:
- Pediatric-type follicular lymphoma: In children, follicular lymphoma occurs mainly in males. It is more likely to be found in one area and does not spread to other places in the body. It usually forms in the tonsils and lymph nodes in the neck, but may also form in the testicles, kidney, gastrointestinal tract, and salivary gland.
- Marginal zone lymphoma: Marginal zone lymphoma is a type of lymphoma that tends to grow and spread slowly and is usually found at an early stage. It may be found in the lymph nodes or in areas outside the lymph nodes. Marginal zone lymphoma found outside the lymph nodes in children is called mucosa-associated lymphoid tissue (MALT) lymphoma. MALT may be linked to Helicobacter pylori infection of the gastrointestinal tract and Chlamydophila psittaci infection of the conjunctival membrane which lines the eye. Marginal zone lymphoma is rare in children but common in adults.
- Primary central nervous system (CNS) lymphoma: Primary CNS lymphoma is extremely rare in children.
- Peripheral T-cell lymphoma: Peripheral T-cell lymphoma is an aggressive (fast-growing) non-Hodgkin lymphoma that begins in mature T lymphocytes. Other types of peripheral T-cell lymphoma include mature T-cell/natural killer-cell lymphoma, extranodal NK/T-cell lymphoma, and gamma-delta hepatosplenic T-cell lymphoma. Peripheral T-cell lymphoma is rare in children.
- Cutaneous T-cell lymphoma: Cutaneous T-cell lymphoma begins in the skin and can cause the skin to thicken or form a tumor. It is very rare in children but is more common in adolescents and young adults. There are different types of cutaneous T-cell lymphoma, such as cutaneous anaplastic large cell lymphoma, subcutaneous panniculitis-like T-cell lymphoma, gamma-delta T-cell lymphoma, and mycosis fungoides. Mycosis fungoides rarely occurs in children and adolescents.
Having a weakened immune system increases the risk of NHL in children.
Anything that increases a person's risk of getting a disease is called a risk factor. Not every child with one or more of these risk factors will develop NHL, and it will develop in some children who don't have any known risk factors. Talk with your child's doctor if you think your child may be at risk.
Some of the types of immune system problems that have been linked with a higher risk of childhood NHL include the following:
- Being infected with the Epstein-Barr virus or human immunodeficiency virus (HIV).
- Having a weakened immune system after a transplant or from medicines given after a transplant.
- Having certain inherited diseases (such as DNA repair defect syndromes which include ataxia-telangiectasia, Nijmegen breakage syndrome, and constitutional mismatch repair deficiency).
- Past treatment for cancer.
If lymphoma or lymphoproliferative disease is linked to a weakened immune system from certain inherited diseases, HIV infection, a transplant or medicines given after a transplant, the condition is called lymphoproliferative disease associated with immunodeficiency. The different types of lymphoproliferative disease associated with immunodeficiency include:
- Lymphoproliferative disease associated with primary immunodeficiency.
- HIV-associated non-Hodgkin lymphoma.
- Post-transplant lymphoproliferative disease.
- Lymphoproliferative disease from chemotherapy.
Signs of childhood non-Hodgkin lymphoma include breathing problems and swollen lymph nodes.
These and other signs may be caused by childhood non-Hodgkin lymphoma or by other conditions. Check with a doctor if your child has any of the following:
- Trouble breathing.
- Wheezing.
- Coughing.
- High-pitched breathing sounds.
- Swelling of the head, neck, upper body, or arms.
- Trouble swallowing.
- Painless swelling of the lymph nodes in the neck, underarm, stomach, or groin.
- Painless lump or swelling in a testicle.
- Fever for no known reason.
- Weight loss for no known reason.
- Drenching night sweats.
- Pain or swelling in the abdomen.
Tests that examine the body and lymph system are used to diagnose childhood non-Hodgkin lymphoma.
In addition to asking about your child's personal and family health history and doing a physical exam, your child's doctor may perform the following tests and procedures:
- Blood chemistry studies: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by organs and tissues in the body, including electrolytes, lactate dehydrogenase (LDH), uric acid, blood urea nitrogen (BUN), creatinine, and liver function values. An unusual (higher or lower than normal) amount of a substance can be a sign of disease.
- Liver function tests: A procedure in which a blood sample is checked to measure the amounts of certain substances released into the blood by the liver. A higher-than-normal amount of a substance can be a sign of cancer.
- CT scan (CAT scan): A procedure that makes a series of detailed pictures of areas inside the body, such as the neck, chest, abdomen, and pelvis, taken from different angles. The pictures are made by a computer linked to an x-ray machine. A dye may be injected into a vein or swallowed to help the organs or tissues show up more clearly. This procedure is also called computed tomography, computerized tomography, or computerized axial tomography.
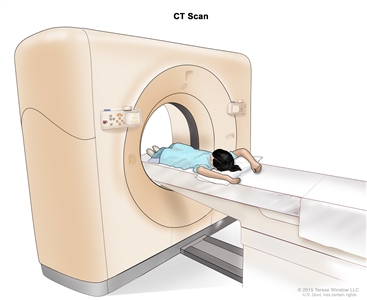
Computed tomography (CT) scan. The child lies on a table that slides through the CT scanner, which takes a series of detailed x-ray pictures of areas inside the body. - PET scan (positron emission tomography scan): A procedure to find malignant tumor cells in the body. A small amount of radioactive glucose (sugar) is injected into a vein. The PET scanner rotates around the body and makes a picture of where glucose is being used in the body. Malignant tumor cells show up brighter in the picture because they are more active and take up more glucose than normal cells do. Sometimes a PET scan and a CT scan are done at the same time. If there is any cancer, this increases the chance that it will be found.
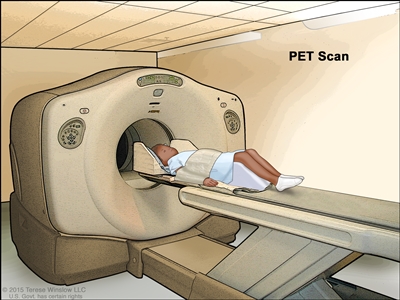
Positron emission tomography (PET) scan. The child lies on a table that slides through the PET scanner. The head rest and white strap help the child lie still. A small amount of radioactive glucose (sugar) is injected into the child's vein, and a scanner makes a picture of where the glucose is being used in the body. Cancer cells show up brighter in the picture because they take up more glucose than normal cells do. - MRI (magnetic resonance imaging): A procedure that uses a magnet, radio waves, and a computer to make a series of detailed pictures of areas inside the body. This procedure is also called nuclear magnetic resonance imaging (NMRI).
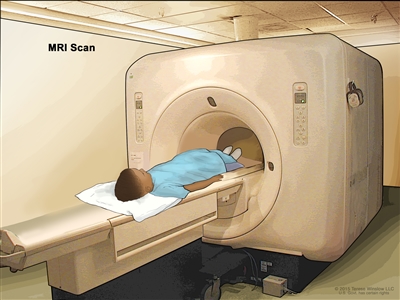
Magnetic resonance imaging (MRI) scan. The child lies on a table that slides into the MRI machine, which takes a series of detailed pictures of areas inside the body. The positioning of the child on the table depends on the part of the body being imaged. - Lumbar puncture: A procedure used to collect cerebrospinal fluid (CSF) from the spinal column. This is done by placing a needle between two bones in the spine and into the CSF around the spinal cord and removing a sample of the fluid. The sample of CSF is checked under a microscope for signs that the cancer has spread to the brain and spinal cord. This procedure is also called an LP or spinal tap.
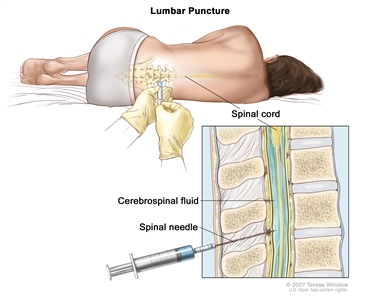
Lumbar puncture. A patient lies in a curled position on a table. After a small area on the lower back is numbed, a spinal needle (a long, thin needle) is inserted into the lower part of the spinal column to remove cerebrospinal fluid (CSF, shown in blue). The fluid may be sent to a laboratory for testing. - Chest x-ray: An x-ray of the organs and bones inside the chest. An x-ray is a type of energy beam that can go through the body and onto film, making a picture of areas inside the body.
- Ultrasound exam: A procedure in which high-energy sound waves (ultrasound) are bounced off internal tissues or organs and make echoes. The echoes form a picture of body tissues called a sonogram.
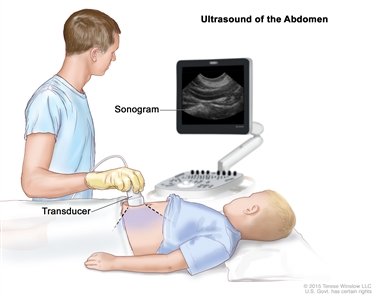
Abdominal ultrasound. An ultrasound transducer connected to a computer is pressed against the skin of the abdomen. The transducer bounces sound waves off internal organs and tissues to make echoes that form a sonogram (computer picture).
A biopsy is done to diagnose childhood non-Hodgkin lymphoma.
Cells and tissues are removed during a biopsy so they can be viewed under a microscope by a pathologist to check for cancer cells. Because treatment depends on the type of non-Hodgkin lymphoma, biopsy samples should be checked by a pathologist who has experience in diagnosing childhood non-Hodgkin lymphoma.
One of the following types of biopsies may be done:
- Excisional biopsy: The removal of an entire lymph node or lump of tissue.
- Incisional biopsy: The removal of part of a lump, lymph node, or sample of tissue.
- Core needle biopsy: The removal of tissue or part of a lymph node using a wide needle.
- Fine-needle aspiration (FNA) biopsy: The removal of tissue or part of a lymph node using a thin needle.
The procedure used to remove the sample of tissue depends on where the tumor is in the body:
- Bone marrow aspiration and biopsy: The removal of bone marrow and a small piece of bone by inserting a hollow needle into the hipbone or breastbone.
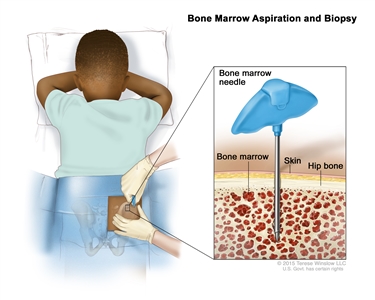
Bone marrow aspiration and biopsy. After a small area of skin is numbed, a bone marrow needle is inserted into the child's hip bone. Samples of blood, bone, and bone marrow are removed for examination under a microscope. - Mediastinoscopy: A surgical procedure to look at the organs, tissues, and lymph nodes between the lungs for abnormal areas. An incision (cut) is made at the top of the breastbone and a mediastinoscope is inserted into the chest. A mediastinoscope is a thin, tube-like instrument with a light and a lens for viewing. It also has a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer.
- Anterior mediastinotomy: A surgical procedure to look at the organs and tissues between the lungs and between the breastbone and heart for abnormal areas. An incision (cut) is made next to the breastbone and a mediastinoscope is inserted into the chest. A mediastinoscope is a thin, tube-like instrument with a light and a lens for viewing. It also has a tool to remove tissue or lymph node samples, which are checked under a microscope for signs of cancer. This is also called the Chamberlain procedure.
- Thoracentesis: The removal of fluid from the space between the lining of the chest and the lung, using a needle. A pathologist views the fluid under a microscope to look for cancer cells.
If cancer is found, the following tests may be done to study the cancer cells:
- Immunohistochemistry: A laboratory test that uses antibodies to check for certain antigens (markers) in a sample of a patient's tissue. The antibodies are usually linked to an enzyme or a fluorescent dye. After the antibodies bind to a specific antigen in the tissue sample, the enzyme or dye is activated, and the antigen can then be seen under a microscope. This type of test is used to help diagnose cancer and to help tell one type of cancer from another type of cancer.
- Flow cytometry: A laboratory test that measures the number of cells in a sample, the percentage of live cells in a sample, and certain characteristics of the cells, such as size, shape, and the presence of tumor (or other) markers on the cell surface. The cells from a sample of a patient's blood, bone marrow, or other tissue are stained with a fluorescent dye, placed in a fluid, and then passed one at a time through a beam of light. The test results are based on how the cells that were stained with the fluorescent dye react to the beam of light. This test is used to help diagnose and manage certain types of cancers, such as leukemia and lymphoma.
- Cytogenetic analysis: A laboratory test in which the chromosomes of cells in a sample of blood or bone marrow are counted and checked for any changes, such as broken, missing, rearranged, or extra chromosomes. Changes in certain chromosomes may be a sign of cancer. Cytogenetic analysis is used to help diagnose cancer, plan treatment, or find out how well treatment is working.
- FISH (fluorescence in situ hybridization): A laboratory test used to look at and count genes or chromosomes in cells and tissues. Pieces of DNA that contain fluorescent dyes are made in the laboratory and added to a sample of a patient's cells or tissues. When these dyed pieces of DNA attach to certain genes or areas of chromosomes in the sample, they light up when viewed under a fluorescent microscope. The FISH test is used to help diagnose cancer and help plan treatment.
- Immunophenotyping: A laboratory test that uses antibodies to identify cancer cells based on the types of antigens or markers on the surface of the cells. This test is used to help diagnose specific types of lymphoma.
Certain factors affect prognosis (chance of recovery) and treatment options.
The prognosis and treatment options depend on:
- The type of lymphoma.
- Where the tumor is in the body when the tumor is diagnosed.
- The stage of the cancer.
- Whether there are certain changes in the chromosomes.
- The type of initial treatment.
- Whether the lymphoma responded to initial treatment.
- The patient's age and general health.
After childhood non-Hodgkin lymphoma has been diagnosed, tests are done to find out if cancer cells have spread within the lymph system or to other parts of the body.
The process used to find out if cancer has spread within the lymph system or to other parts of the body is called staging. The results of tests and procedures used to diagnose non-Hodgkin lymphoma may also be used for staging. The information gathered from the staging process determines the stage of the disease. It is important to know the stage in order to plan treatment.
For a description of the tests and procedures used to diagnose non-Hodgkin lymphoma, see General Information.
There are three ways that cancer spreads in the body.
Cancer can spread through tissue, the lymph system, and the blood:
- Tissue. The cancer spreads from where it began by growing into nearby areas.
- Lymph system. The cancer spreads from where it began by getting into the lymph system. The cancer travels through the lymph vessels to other parts of the body.
- Blood. The cancer spreads from where it began by getting into the blood. The cancer travels through the blood vessels to other parts of the body.
The following stages are used for childhood non-Hodgkin lymphoma:
Stage I
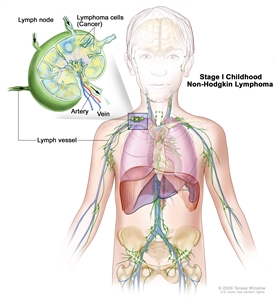
Stage I childhood non-Hodgkin lymphoma. Cancer is found in one group of lymph nodes or one area outside the lymph nodes, but no cancer is found in the abdomen or mediastinum (area between the lungs).
In stage I childhood non-Hodgkin lymphoma, cancer is found:
- in one group of lymph nodes; or
- in one area outside the lymph nodes.
No cancer is found in the abdomen or mediastinum (area between the lungs).
Stage II
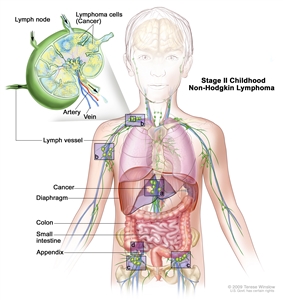
Stage II childhood non-Hodgkin lymphoma. Cancer is found in one area outside the lymph nodes and in nearby lymph nodes (a); or in two or more areas above (b) or below (c) the diaphragm; or cancer started in the stomach, appendix, or intestines (d) and can be removed by surgery.
In stage II childhood non-Hodgkin lymphoma, cancer is found:
- in one area outside the lymph nodes and in nearby lymph nodes; or
- in two or more areas either above or below the diaphragm, and may have spread to nearby lymph nodes; or
- to have started in the stomach or intestines and can be completely removed by surgery. Cancer may have spread to certain nearby lymph nodes.
Stage III
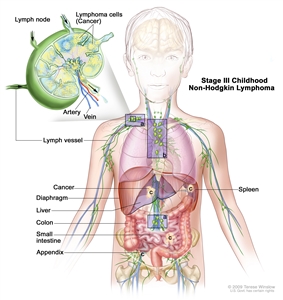
Stage III childhood non-Hodgkin lymphoma. Cancer is found in at least one area above and below the diaphragm (a); or cancer started in the chest (b); or cancer started in the abdomen and spread throughout the abdomen (c); or in the area around the spine (not shown).
In stage III childhood non-Hodgkin lymphoma, cancer is found:
- in at least one area above the diaphragm and in at least one area below the diaphragm; or
- to have started in the chest; or
- to have started in the abdomen and spread throughout the abdomen and cannot be completely removed by surgery; or
- in the area around the spine.
Stage IV
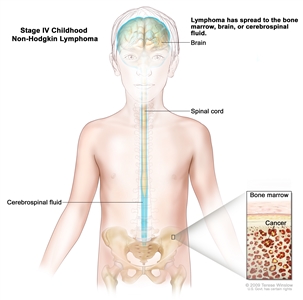
Stage IV childhood non-Hodgkin lymphoma. Cancer is found in the bone marrow, brain, or cerebrospinal fluid (CSF). Cancer may also be found in other parts of the body.
In stage IV childhood non-Hodgkin lymphoma, cancer is found in the bone marrow, brain, or cerebrospinal fluid. Cancer may also be found in other parts of the body.
Sometimes childhood non-Hodgkin lymphoma does not respond to treatment or recurs (comes back) after treatment.
Refractory non-Hodgkin lymphoma is cancer that does not respond to initial treatment.
Recurrent non-Hodgkin lymphoma is cancer that has come back after treatment. It may come back in the lymph system or in other parts of the body.
There are different types of treatment for children with non-Hodgkin lymphoma.
Different types of treatment are available for children with non-Hodgkin lymphoma. Some treatments are standard (the currently used treatment), and some are being tested in clinical trials. A treatment clinical trial is a research study meant to help improve current treatments or obtain information on new treatments for patients with cancer. When clinical trials show that a new treatment is better than the standard treatment, the new treatment may become the standard treatment.
Taking part in a clinical trial should be considered for all children with non-Hodgkin lymphoma. Some clinical trials are open only to patients who have not started treatment.
Children with non-Hodgkin lymphoma should have their treatment planned by a team of doctors who are experts in treating childhood cancer.
Treatment will be overseen by a pediatric oncologist, a doctor who specializes in treating children with cancer. The pediatric oncologist works with other health care providers who are experts in treating children with non-Hodgkin lymphoma and who specialize in certain areas of medicine. These may include the following specialists:
- Pediatrician.
- Radiation oncologist.
- Pediatric hematologist.
- Pediatric surgeon.
- Pediatric nurse specialist.
- Rehabilitation specialist.
- Psychologist.
- Social worker.
Eight types of treatment are used:
Surgery
Surgery may be done to remove as much of the tumor as possible for some types of childhood non-Hodgkin lymphoma. After the doctor removes all the cancer that can be seen at the time of surgery, patients may be given chemotherapy to kill any cancer cells that are left. Treatment given after the surgery, to lower the risk that the cancer will come back, is called adjuvant therapy.
Chemotherapy
Chemotherapy is a cancer treatment that uses drugs to stop the growth of cancer cells, either by killing the cells or by stopping them from dividing. When chemotherapy is taken by mouth or injected into a vein or muscle, the drugs enter the bloodstream and can reach cancer cells throughout the body (systemic chemotherapy). When chemotherapy is placed directly into the cerebrospinal fluid (intrathecal chemotherapy), an organ, or a body cavity such as the abdomen, the drugs mainly affect cancer cells in those areas. Combination chemotherapy is treatment using two or more anticancer drugs.
Intrathecal chemotherapy may be used to treat childhood non-Hodgkin lymphoma that has spread, or may spread, to the brain. When used to lessen the chance cancer will spread to the brain, it is called CNS prophylaxis. Intrathecal chemotherapy is given in addition to chemotherapy by mouth or vein. Higher than usual doses of chemotherapy may also be used as CNS prophylaxis.
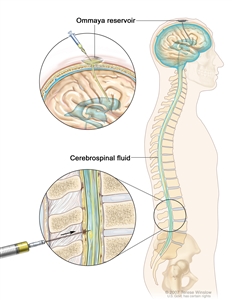
Intrathecal chemotherapy. Anticancer drugs are injected into the intrathecal space, which is the space that holds the cerebrospinal fluid (CSF, shown in blue). There are two different ways to do this. One way, shown in the top part of the figure, is to inject the drugs into an Ommaya reservoir (a dome-shaped container that is placed under the scalp during surgery; it holds the drugs as they flow through a small tube into the brain). The other way, shown in the bottom part of the figure, is to inject the drugs directly into the CSF in the lower part of the spinal column, after a small area on the lower back is numbed.
The way the chemotherapy is given depends on the type and stage of the cancer being treated.
For more information, see Drugs Approved for Non-Hodgkin Lymphoma.
Radiation therapy
Radiation therapy is a cancer treatment that uses high energy x-rays or other types of radiation to kill cancer cells or keep them from growing. External radiation therapy uses a machine outside the body to send radiation toward the area of the body with cancer. External radiation therapy may be used to treat childhood non-Hodgkin lymphoma that has spread, or may spread, to the brain and spinal cord. External radiation therapy may also be used to treat cutaneous T-cell lymphoma (mycosis fungoides).
High-dose chemotherapy with stem cell transplant
High doses of chemotherapy are given to kill cancer cells. Healthy cells, including blood -forming cells, are also destroyed by the cancer treatment. Stem cell transplant is a treatment to replace the blood-forming cells. Stem cells (immature blood cells) are removed from the blood or bone marrow of the patient or a donor and are frozen and stored. After the patient completes chemotherapy, the stored stem cells are thawed and given to the patient through an infusion. These reinfused stem cells grow into (and restore) the body's blood cells.
For more information, see Drugs Approved for Non-Hodgkin Lymphoma.
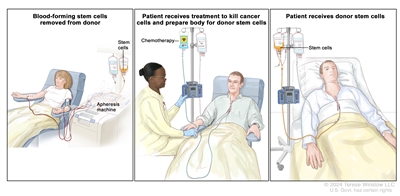
Donor stem cell transplant. (Step 1): Four to five days before donor stem cell collection, the donor receives a medicine to increase the number of stem cells circulating through their bloodstream (not shown). The blood-forming stem cells are then collected from the donor through a large vein in their arm. The blood flows through an apheresis machine that removes the stem cells. The rest of the blood is returned to the donor through a vein in their other arm. (Step 2): The patient receives chemotherapy to kill cancer cells and prepare their body for the donor stem cells. The patient may also receive radiation therapy (not shown). (Step 3): The patient receives an infusion of the donor stem cells.
Targeted therapy
Targeted therapy uses drugs or other substances to block the action of specific enzymes, proteins, or other molecules involved in the growth and spread of cancer cells. Types of targeted therapy include the following:
- Monoclonal antibody therapy: Monoclonal antibodies are immune system proteins made in the laboratory to treat many diseases, including cancer. As a cancer treatment, these antibodies can attach to a specific target on cancer cells or other cells that may help cancer cells grow. The antibodies are able to then kill the cancer cells, block their growth, or keep them from spreading. Monoclonal antibodies are given by infusion. They may be used alone or to carry drugs, toxins, or radioactive material directly to cancer cells. Monoclonal antibodies may be used in combination with chemotherapy as adjuvant therapy.
Types of monoclonal antibodies include:
- Rituximab is used to treat several types of childhood non-Hodgkin lymphoma.
- Pembrolizumab is used to treat primary mediastinal large B-cell lymphoma that has not responded to treatment or has recurred (come back). Treatment with pembrolizumab has been mostly studied in adults.
- Brentuximab vedotin is a monoclonal antibody combined with an anticancer drug that is used to treat anaplastic large cell lymphoma that has not responded to treatment or has recurred.
- A bispecific monoclonal antibody is made up of two different monoclonal antibodies that bind to two different substances and kills cancer cells. Bispecific monoclonal antibody therapy is used in the treatment of Burkitt lymphoma/leukemia and diffuse large B-cell lymphoma that have not responded to treatment or have recurred.
- Nivolumab is being studied in the treatment of anaplastic large cell lymphoma with a certain gene change that has not responded to treatment or has recurred.
- ALK inhibitor therapy: ALK inhibitors block the activity of a protein called anaplastic lymphoma kinase. Blocking this protein may help keep cancer cells from growing and spreading. Crizotinib, alectinib, and ceritinib may be used to treat anaplastic large cell lymphoma that has not responded to treatment or has recurred. Crizotinib is also being studied in the treatment of newly diagnosed anaplastic large cell lymphoma.
- Proteasome inhibitor therapy: This treatment blocks the actions of proteasomes in cancer cells. Proteasomes remove proteins no longer needed by the cell. When the proteasomes are blocked, the protons build up in the cell and may cause the cancer cell to die. Bortezomib may be used to treat lymphoblastic lymphoma that has not responded to treatment or has recurred.
- Immunotoxins: This treatment can bind to cancer cells and kill them. Denileukin diftitox is an immunotoxin used to treat cutaneous T-cell lymphoma.
Other targeted therapies are being studied for the treatment of childhood non-Hodgkin lymphoma that has not responded to treatment or has recurred (come back).
For more information, see Drugs Approved for Non-Hodgkin Lymphoma.
Other drug therapy
Retinoids are drugs related to vitamin A. Retinoid therapy with bexarotene is used to treat several types of cutaneous T-cell lymphoma.
Steroids are hormones made naturally in the body. They can also be made in a laboratory and used as drugs. Steroid therapy that is applied to the skin is used to treat cutaneous T-cell lymphoma. Dexamethasone and prednisone are steroids used with other drugs to treat certain types of lymphoma.
Antibiotics are drugs used to treat infections and cancer caused by bacteria or other microorganisms. Antibiotics have been used to treat mucosa-associated lymphoid tissue (MALT) lymphoma. Treatment with antibiotic therapy has been mostly studied in adults.
Phototherapy
Phototherapy is a cancer treatment that uses a drug and a certain type of laser light to kill cancer cells. A drug that is not active until it is exposed to light is injected into a vein. The drug collects more in cancer cells than in normal cells. For skin cancer in the skin, laser light is shined onto the skin and the drug becomes active and kills the cancer cells. Phototherapy is used in the treatment of cutaneous T-cell lymphoma.
Watchful waiting
Watchful waiting is closely monitoring a patient's condition without giving any treatment until signs or symptoms appear or change.
New types of treatment are being tested in clinical trials.
This summary section describes treatments that are being studied in clinical trials. It may not mention every new treatment being studied. Information about clinical trials is available from the NCI website.
Immunotherapy
Immunotherapy helps a person's immune system fight cancer. Types of immunotherapy include:
- CAR T-cell therapy: This treatment changes the patient's T cells (a type of immune system cell) so they will attack certain proteins on the surface of cancer cells. T cells are taken from the patient and special receptors are added to their surface in the laboratory. The changed cells are called chimeric antigen receptor (CAR) T cells. The CAR T cells are grown in the laboratory and given to the patient by infusion. The CAR T cells multiply in the patient's blood and attack cancer cells. CAR T-cell therapy is being studied in the treatment of Burkitt lymphoma/leukemia and diffuse large B-cell lymphoma that has not responded to treatment or has recurred (come back).
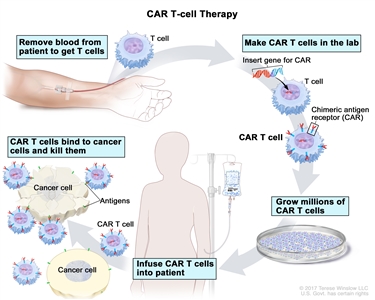
CAR T-cell therapy. A type of treatment in which a patient's T cells (a type of immune cell) are changed in the laboratory so they will bind to cancer cells and kill them. Blood from a vein in the patient's arm flows through a tube to an apheresis machine (not shown), which removes the white blood cells, including the T cells, and sends the rest of the blood back to the patient. Then, the gene for a special receptor called a chimeric antigen receptor (CAR) is inserted into the T cells in the laboratory. Millions of the CAR T cells are grown in the laboratory and then given to the patient by infusion. The CAR T cells are able to bind to an antigen on the cancer cells and kill them. - Epstein-Barr virus (EBV)-specific cytotoxic T-lymphocytes are a type of immune cell that can kill certain cells, including foreign cells, cancer cells, and cells infected with the EBV. Cytotoxic T-lymphocytes can be separated from other blood cells, grown in the laboratory, and then given to the patient to kill cancer cells. EBV-specific cytotoxic T-lymphocytes are being studied to treat post-transplant lymphoproliferative disease.
- Cyclosporine A: This treatment is used in combination with steroids to treat subcutaneous panniculitic T-cell lymphoma.
Treatment for childhood non-Hodgkin lymphoma may cause side effects.
To learn more about side effects that begin during treatment for cancer, visit Side Effects.
Side effects from cancer treatment that begin after treatment and continue for months or years are called late effects. Late effects of cancer treatment may include the following:
- Physical problems, including problems with the heart, bones, and fertility.
- Changes in mood, feelings, thinking, learning, or memory.
- Second cancers (new types of cancer), such as brain tumors, acute myeloid leukemia, and myelodysplastic syndrome.
Some late effects may be treated or controlled. It is important to talk with your child's doctors about the effects cancer treatment can have on your child. For more information, see Late Effects of Treatment for Childhood Cancer.
Patients may want to think about taking part in a clinical trial.
For some patients, taking part in a clinical trial may be the best treatment choice. Clinical trials are part of the cancer research process. Clinical trials are done to find out if new cancer treatments are safe and effective or better than the standard treatment.
Many of today's standard treatments for cancer are based on earlier clinical trials. Patients who take part in a clinical trial may receive the standard treatment or be among the first to receive a new treatment.
Patients who take part in clinical trials also help improve the way cancer will be treated in the future. Even when clinical trials do not lead to effective new treatments, they often answer important questions and help move research forward.
Patients can enter clinical trials before, during, or after starting their cancer treatment.
Some clinical trials only include patients who have not yet received treatment. Other trials test treatments for patients whose cancer has not gotten better. There are also clinical trials that test new ways to stop cancer from recurring (coming back) or reduce the side effects of cancer treatment.
Clinical trials are taking place in many parts of the country. Information about clinical trials supported by NCI can be found on NCI's clinical trials search webpage. Clinical trials supported by other organizations can be found on the ClinicalTrials.gov website.
Follow-up tests may be needed.
As your child goes through treatment, they will have follow-up tests or check-ups. Some tests that were done to diagnose or stage the cancer may be repeated to see how well the treatment is working. Decisions about whether to continue, change, or stop treatment may be based on the results of these tests.
Some of the tests will continue to be done from time to time after treatment has ended. The results of these tests can show if your child's condition has changed or if the cancer has recurred (come back).
Burkitt lymphoma/leukemia
Treatment of Burkitt lymphoma/leukemia
For information about the treatments listed below, see Treatment Option Overview.
Treatment of newly diagnosed Burkitt lymphoma /leukemia may include:
- Surgery to remove as much of the tumor as possible, followed by combination chemotherapy.
- Combination chemotherapy with or without targeted therapy (rituximab).
Treatment of recurrent or refractory Burkitt lymphoma/leukemia
For information about the treatments listed below, see Treatment Option Overview.
Treatment of recurrent or refractory Burkitt lymphoma /leukemia may include:
- Combination chemotherapy with or without targeted therapy (rituximab).
- Targeted therapy (rituximab), combination chemotherapy, and dexamethasone.
- High-dose chemotherapy with stem cell transplant with the patient's own cells or cells from a donor.
- Targeted therapy with a bispecific antibody.
- CAR T-cell therapy.
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Diffuse large B-cell lymphoma
Treatment of diffuse large B-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of newly diagnosed diffuse large B-cell lymphoma may include:
- Surgery to remove as much of the tumor as possible, followed by combination chemotherapy.
- Combination chemotherapy with or without targeted therapy (rituximab).
Treatment of recurrent or refractory diffuse large B-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of recurrent or refractory diffuse large B-cell lymphoma may include:
- Combination chemotherapy with or without targeted therapy (rituximab).
- Targeted therapy (rituximab), combination chemotherapy, and dexamethasone.
- High-dose chemotherapy with stem cell transplant with the patient's own cells or cells from a donor.
- Targeted therapy with a bispecific antibody.
- CAR T-cell therapy.
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Primary Mediastinal B-cell Lymphoma
Treatment of primary mediastinal B-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of newly diagnosed primary mediastinal B-cell lymphoma may include:
- Combination chemotherapy, prednisone, and targeted therapy (rituximab).
- A clinical trial of combination chemotherapy, prednisone, and targeted therapy (rituximab) with or without an additional targeted therapy (nivolumab).
Treatment of recurrent or refractory primary mediastinal B-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of recurrent or refractory primary mediastinal B-cell lymphoma may include:
- Targeted therapy (pembrolizumab).
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Lymphoblastic Lymphoma
Treatment of lymphoblastic lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Lymphoblastic lymphoma may be classified as the same disease as acute lymphoblastic leukemia (ALL). Treatment of lymphoblastic lymphoma may include:
- Combination chemotherapy.
- CNS prophylaxis with radiation therapy may also be given if cancer has spread to the brain or spinal cord.
Treatment of recurrent or refractory lymphoblastic lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of recurrent or refractory lymphoblastic lymphoma may include:
- Chemotherapy.
- Targeted therapy (bortezomib) with combination chemotherapy.
- High-dose chemotherapy with stem cell transplant with cells from a donor.
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Anaplastic Large Cell Lymphoma
Treatment of anaplastic large cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of anaplastic large cell lymphoma may include:
- Surgery followed by combination chemotherapy.
- Combination chemotherapy with or without prednisone.
- Intrathecal and combination chemotherapy, for patients with cancer in the brain or spinal cord.
Treatment of recurrent or refractory anaplastic large cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of recurrent or refractory anaplastic large cell lymphoma may include:
- Chemotherapy, brentuximab, crizotinib, alectinib, and/or ceritinib.
- Stem cell transplant with the patient's own cells or cells from a donor.
- Radiation therapy or high-dose chemotherapy for patients whose disease progresses to the central nervous system.
- A clinical trial of targeted therapy (nivolumab).
- A clinical trial that checks a sample of the patient's tumor for certain gene changes. The type of targeted therapy that will be given to the patient depends on the type of gene change.
Use our clinical trial search to find NCI-supported cancer clinical trials that are accepting patients. You can search for trials based on the type of cancer, the age of the patient, and where the trials are being done. General information about clinical trials is also available.
Lymphoproliferative Disease Associated With Immunodeficiency in Children
Treatment of lymphoproliferative disease associated with primary immunodeficiency
For information about the treatments listed below, see Treatment Option Overview.
Treatment of lymphoproliferative disease in children and adolescents with weakened immune systems may include:
- Chemotherapy with or without rituximab.
- Stem cell transplant with cells from a donor may be used to treat the primary immunodeficiency. This treatment decreases the risk of the cancer recurring (coming back).
Treatment of non-Hodgkin lymphoma associated with DNA repair defect syndromes
For information about the treatments listed below, see Treatment Option Overview.
Treatment of non-Hodgkin lymphoma associated with DNA repair defect syndromes in children may include:
- Chemotherapy.
Treatment of HIV-associated non-Hodgkin lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment with highly active antiretroviral therapy or HAART (a combination of antiretroviral drugs) lowers the risk of non-Hodgkin lymphoma in patients infected with the human immunodeficiency virus (HIV).
Treatment of HIV-related non-Hodgkin lymphoma (NHL) in children may include:
- Chemotherapy with or without rituximab.
For treatment of recurrent disease, treatment options depend on the type of non-Hodgkin lymphoma.
Treatment of post-transplant lymphoproliferative disease
For information about the treatments listed below, see Treatment Option Overview.
Treatment of post-transplant lymphoproliferative disease may include:
- Surgery to remove the tumor. If possible, lower doses of immunosuppressive drugs after a stem cell or organ transplant may be given.
- Targeted therapy (rituximab).
- Chemotherapy with or without targeted therapy (rituximab).
- A treatment of immunotherapy using donor lymphocytes or the patient's own T cells to target Epstein-Barr infection is being studied. This treatment is only available at a few centers in the United States.
Rare NHL Occurring in Children
Treatment of pediatric-type follicular lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of follicular lymphoma in children may include:
- Surgery.
- Combination chemotherapy with or without rituximab.
For children whose cancer has certain changes in the genes, treatment is similar to that given to adults with follicular lymphoma. For information about the treatment of follicular lymphoma in adults, see Adult Non-Hodgkin Lymphoma.
Treatment of marginal zone lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of marginal zone lymphoma (including mucosa-associated lymphoid tissue [MALT] lymphoma) in children may include:
- Surgery.
- Radiation therapy.
- Rituximab with or without chemotherapy.
- Antibiotic therapy, for MALT lymphoma.
Treatment of primary CNS lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of primary CNS lymphoma in children may include:
- Chemotherapy.
Treatment of peripheral T-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of peripheral T-cell lymphoma in children may include:
- Chemotherapy.
- Radiation therapy.
- Stem cell transplant with the patient's own cells or cells from a donor.
Treatment of cutaneous T-cell lymphoma
For information about the treatments listed below, see Treatment Option Overview.
Treatment of subcutaneous panniculitis-like T-cell lymphoma in children may include:
- Watchful waiting.
- Immunotherapy using high-dose steroids with or without cyclosporine A or ruxolitinib.
- Targeted therapy (denileukin diftitox).
- Combination chemotherapy.
- Retinoid therapy.
- Stem cell transplant.
Treatment of cutaneous anaplastic large cell lymphoma may include:
- Surgery, radiation therapy, or both.
Treatment of mycosis fungoides
For information about the treatments listed below, see Treatment Option Overview.
In children, treatment of mycosis fungoides may include:
- Steroids applied to the skin.
- Retinoid therapy.
- Radiation therapy.
- Phototherapy (light therapy using ultraviolet B radiation).
For more information from the National Cancer Institute about childhood non-Hodgkin lymphoma, see the following:
- Computed Tomography (CT) Scans and Cancer
- Drugs Approved for Non-Hodgkin Lymphoma
- Blood-Forming Stem Cell Transplants
- Targeted Therapy to Treat Cancer
- Immunotherapy to Treat Cancer
For more childhood cancer information and other general cancer resources, visit:
- About Cancer
- Childhood Cancers
- CureSearch for Children's Cancer
- Late Effects of Treatment for Childhood Cancer
- Adolescents and Young Adults with Cancer
- Children with Cancer: A Guide for Parents
- Cancer in Children and Adolescents
- Staging
- Coping with Cancer
- Questions to Ask Your Doctor about Cancer
- For Survivors and Caregivers
About PDQ
Physician Data Query (PDQ) is the National Cancer Institute's (NCI's) comprehensive cancer information database. The PDQ database contains summaries of the latest published information on cancer prevention, detection, genetics, treatment, supportive care, and complementary and alternative medicine. Most summaries come in two versions. The health professional versions have detailed information written in technical language. The patient versions are written in easy-to-understand, nontechnical language. Both versions have cancer information that is accurate and up to date and most versions are also available in Spanish.
PDQ is a service of the NCI. The NCI is part of the National Institutes of Health (NIH). NIH is the federal government's center of biomedical research. The PDQ summaries are based on an independent review of the medical literature. They are not policy statements of the NCI or the NIH.
Purpose of This Summary
This PDQ cancer information summary has current information about the treatment of childhood non-Hodgkin lymphoma. It is meant to inform and help patients, families, and caregivers. It does not give formal guidelines or recommendations for making decisions about health care.
Reviewers and Updates
Editorial Boards write the PDQ cancer information summaries and keep them up to date. These Boards are made up of experts in cancer treatment and other specialties related to cancer. The summaries are reviewed regularly and changes are made when there is new information. The date on each summary ("Updated") is the date of the most recent change.
The information in this patient summary was taken from the health professional version, which is reviewed regularly and updated as needed, by the PDQ Pediatric Treatment Editorial Board.
Clinical Trial Information
A clinical trial is a study to answer a scientific question, such as whether one treatment is better than another. Trials are based on past studies and what has been learned in the laboratory. Each trial answers certain scientific questions in order to find new and better ways to help cancer patients. During treatment clinical trials, information is collected about the effects of a new treatment and how well it works. If a clinical trial shows that a new treatment is better than one currently being used, the new treatment may become "standard." Patients may want to think about taking part in a clinical trial. Some clinical trials are open only to patients who have not started treatment.
Clinical trials can be found online at NCI's website. For more information, call the Cancer Information Service (CIS), NCI's contact center, at 1-800-4-CANCER (1-800-422-6237).
Permission to Use This Summary
PDQ is a registered trademark. The content of PDQ documents can be used freely as text. It cannot be identified as an NCI PDQ cancer information summary unless the whole summary is shown and it is updated regularly. However, a user would be allowed to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks in the following way: [include excerpt from the summary]."
The best way to cite this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Non-Hodgkin Lymphoma Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/lymphoma/patient/child-nhl-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389294]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use in the PDQ summaries only. If you want to use an image from a PDQ summary and you are not using the whole summary, you must get permission from the owner. It cannot be given by the National Cancer Institute. Information about using the images in this summary, along with many other images related to cancer can be found in Visuals Online. Visuals Online is a collection of more than 3,000 scientific images.
Disclaimer
The information in these summaries should not be used to make decisions about insurance reimbursement. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's E-mail Us.
Last Revised: 2023-07-27
If you want to know more about cancer and how it is treated, or if you wish to know about clinical trials for your type of cancer, you can call the NCI's Cancer Information Service at 1-800-422-6237, toll free. A trained information specialist can talk with you and answer your questions.
This information does not replace the advice of a doctor. Ignite Healthwise, LLC, disclaims any warranty or liability for your use of this information. Your use of this information means that you agree to the Terms of Use. Learn how we develop our content.