Since 2004, the U-M Health System has been in the national spotlight for its innovative approach to medical errors, mishaps and near-misses -- and their potential legal consequences including malpractice suits. We call it the Michigan Model.
In May 2016, the Agency for Healthcare Research and Quality introduced the CANDOR Toolkit, a free resource to help hospitals adopt this same approach. Based in part on our model, it was built using expert input and lessons learned from the agency's $23 million Patient Safety and Medical Liability grant initiative launched in 2009, and was tested and applied in 14 hospitals across three U.S. health systems.
Read our writeup about this resource: Hospitals Can Break Through the 'Wall of Silence' with New Toolkit
What is the Michigan Model?
It's our approach to medical errors and malpractice claims. Click here to jump down to a summary.
See below for more links to resources and news coverage related to this issue, including testimony and articles.
It's important to note that our approach to medical malpractice claims is closely linked with our innovative approach to patient safety. For more on that, see our Quality and Safety Web site.
Reporters interested in learning more about our programs or interviewing Executive Director for Clinical Safety and Chief Risk Officer Rick Boothman, J.D., may contact Kara Gavin, UMHS Dept. of Communication, at 734-764-2220.
Publications about the Michigan Model:
- Joint Commission Journal on Quality and Patient Safety editorial, April 2016: Breaking Through Dangerous Silence to Tap an Organization’s
Richest Source of Information: Its Own Staff (available upon request)
- Case Study 1, National Patient Safety Foundation Lucian Leape Institute report, January 2015: "Shining a Light: Safer Health Care Through Transparency"
- Health Affairs, January 2014 - Communication-And-Resolution Programs: The Challenges and Lessons Learned from Six Early Adopters
- American Journal of Gastroenterology, November 2013 - Effect of a Health System's Medical Error Disclosure Program on Gastroenterology-Related Claims Rates and Costs
- Bulletin of the American College of Surgeons, March 2013 - The University of Michigan's Early Disclosure & Offer Program
- Milbank Quarterly, December 2012 - Disclosure, Apology, and Offer Programs: Stakeholders' Views of Barriers to and Strategies for Broad Implementation
- Press release: Doing the right thing when things go wrong
- Frontiers in Health Services Management, April 2012 - Nurturing a Culture of Patient Safety and Achieving Lower Malpractice Risk Through Disclosure: Lessons Learned and Future Directions
- Annals of Internal Medicine, August 2010 - Liability Claims and Costs Before and After Implementation of a Medical Error Disclosure Program
- Journal of Health and Life Sciences Law, January 2009 - A Better Approach to Medical Malpractice Claims? The University of Michigan Experience
Online resources:
FREE TOOLKIT FOR HOSPITALS: Agency for Healthcare Research & Quality CANDOR Toolkit
VIDEO: CANDOR Toolkit, Agency for Healthcare Research and Quality - Rick Boothman and others
VIDEO: 2014 Patient Safety Summit - Culture of Safety Panel (Rick Boothman remarks)
VIDEO: MITSS 2013 Annual Dinner - keynote address by Rick Boothman
Massachusetts Medical Society: Physicians, Hospitals, Health Groups announce initiative to improve the medical liability environment in Massachusetts (Mass. Medical Society press release)
“Medical Justice: Making the System Work Better for Patients and Doctors (PDF)” - Testimony of Rick Boothman before the U.S. Senate Committee on Health, Education, Labor and Pensions, June 22, 2006
"Making Patient Safety the Centerpiece of Medical Liability Reform" - New England Journal of Medicine Perspective article by Senators Hillary Rodham Clinton and Barack Obama (Volume 354 Number 21 :2205-2208 ) May 25, 2006. Audio interview related to NEJM article, featuring Rick Boothman
Transparency: The Benefits of an Open and Honest Dialogue (PPT)
Powerpoint presentation given by Rick Boothman to the Health Law Division of the State Bar of Michigan, April 26, 2006 (11.1 MB download)
Articles and news items on our approach:
Hospitals Can Break Through the ‘Wall of Silence’ with New Toolkit, Michigan Health Lab, May 23, 2016
The 'Michigan Model' for Malpractice Reform: Wall Street Journal (opinion), May 10, 2015 (subscription required)
Service Members are Left in Dark on Health Errors: New York Times, April 19, 2015
Mass. Malpractice Reforms Offer Faster, More Open Process for Injured Patients, Kaiser Health News, January 20, 2015
The Transformative Power of Transparency: New York Times Dealbook blog by Dov Seidman, May 23, 2014
The Honesty Policy: Ann Arbor Observer, May 2014
Making Apologies in Healthcare Advance for Nurse Practitioners and Physician Assistants
October 20134 Tips to Implement a Transparent Medical Error Disclosure Policy Becker's Hospital Review, July 2013
The Dogmas of the Past are Inadequate - Islands of Excellence blog, May 2013
Lessons from America's Safest Hospitals
AARP Magazine April, 2013UMHS malpractice approach wins praise
Michigan Daily January 11, 2013One doctor’s take on malpractice policy that calls for disclosure, apology, and often a settlement
Boston Globe April 23, 2012When Doctors Admit Their Mistakes
New York Times Aug. 19, 2010Admitting errors doesn't increase lawsuits: study
Reuters Health Aug 17, 2010What happens to liability costs when a hospital admits errors?
Wall Street Journal Aug. 16, 2010When doctors admit mistakes, fewer malpractice suits result, study says HealthDay
Aug. 17, 2010Our view on doctors vs. lawyers: Tired malpractice debate ignores promising solutions USA Today
June 22, 2009Hospitals Find Confession Good for the Bottom Line Crain's Detroit Business
May 10, 2009Doctors Say ‘I’m Sorry’ Before ‘See You in Court’ New York Times
May 18, 2008Practice of Hospital Apologies Is Gaining Ground National Public Radio, All Things Considered
Oct. 6, 2007Doctors try a new word: Sorry Fuller disclosure of errors is changing the culture of secrecy in medicine. Chicago Tribune, Sept. 2007 Available online via the Orange County Register
Doctors Learn to Say 'I'm Sorry', Informed Patient Column, Wall Street Journal, Jan. 24, 2007(Available online to subscribers only)
Curing the Malpractice Crisis by RIck Boothman, Guest opinion - Surgery News, page 12, August 2006
The Medical Malpractice Myth, by Ezra Klein - The Slate, July 11, 2006
Column by Rick Boothman and Dr. Steve Kraman, former chief of staff, Lexington, Ky. Veterans Affairs medical center (posted on the SorryWorks! Coalition Web site)
Apologies and a Strong Defense at the University of Michigan Health System The Physician Executive March/April 2006 edition (see page 2 of the PDF)
Saying ‘I’m Sorry’ Is Starting to Pay Off with Reduced Lawsuits and Legal Costs Healthcare Risk Management, October 2005
National Public Radio interview with Rick Boothman – December 2004
Copies of other news articles are available upon request from Kara Gavin, UMHS Dept. of Communication, 734-764-2220.
The Michigan Model:
The U-M Health System approach to medical errors, near misses and malpractice claims
There’s something different going on at the University of Michigan Health System when it comes to patient safety, medical mishaps and medical malpractice litigation.
You may have heard something about our policy of “saying sorry”, or apologizing and having an open discussion, when clinical care does not go as planned. And while apologies are certainly part of our approach, there’s much more to it than that. Communication, full disclosure, and learning from our experiences are all vital.
You may have also heard that we have steadily reduced the number of malpractice claims pending against us and our doctors, slashed our malpractice expenses, dramatically dropped the amount paid to plaintiffs as a result of judgments or settlements, and cut the time it takes to handle a claim. All of this is true.
In short, we’re trying to “do the right thing” for our patients, our medical staff, and the public interest. We believe that court should be the last resort, not the first, when a medical mishap, complication or near-miss occurs.
This page will help you understand our approach, and what we have achieved in the years since we began using it. We don’t claim to have all the answers. But we hope this information will be useful to other health care institutions, as well as the news media, as we all grapple with medical errors and the current malpractice climate.
First, some important background information:
- UMHS has committed itself to being one of the safest medical centers in America, and to a constant search for new ways to prevent errors, infections, patient and staff injuries, and near-misses. And when a mishap or near-miss occurs, we’re committed to confronting its causes in a blame-free way, and learning from it so that it doesn’t happen again.
- We’re fortunate to be located in Michigan, a state that passed sensible medical malpractice reform in the 1990s and is not having some of the same crisis situations as other states. Our state law, among other things, builds a six-month “cooling off” period into the malpractice lawsuit process. If a patient is thinking about bringing suit against a doctor or hospital for medical malpractice, the patient must first alert prospective defendants of their complaints with a “notice of intent,” and both parties then have six months to consider their cases before going to court. UMHS systematically uses that period to investigate complaints and establish a dialogue with our patients, and their attorneys if they are represented, which often eliminates their need to resort to litigation.
- We’re self-insured for malpractice insurance. All of the U-M physicians who treat patients at the U-M Hospitals & Health Centers are also faculty of our Medical School, and part of our Michigan Medical Group practice. The U-M General Counsel manages all claims against our medical staff, through staff and outside attorneys.
- We have excellent faculty and staff who provide some of the most complex, advanced medical care in the United States, from transplants of bone marrow and organs, to complex cancer regimens, to open-heart surgery on newborn babies. As a result, our patient population on the whole has more serious and more complex medical issues than the populations at other hospitals. And we’re attracting more patients than ever. This combination of factors means that we walk a high tightrope of risk every day. While independent measures show that our care is world-class, we face the reality that complications can happen despite our best efforts, that procedures and treatments carry risks, and that we must always search for ways to control factors that can affect our patients’ outcomes.
So, what do we do when something happens that shouldn’t have?
How exactly do we handle malpractice suits?
And what results have this novel approach yielded?
Our approach can be summarized as:
“Apologize and learn when we’re wrong, explain and vigorously defend when we’re right, and view court as a last resort.”
We care deeply about our patients, and we take it very seriously when one of them is injured, concerned or unhappy about the care we have provided. We also care deeply about our staff, and we want to support and protect them so they can continue to do great work. And, we want to create as safe an environment as possible for both patients and staff.
So, when a patient complains, or a staff person realizes that a mishap or near miss has occurred, several things happen:
- We follow our institutional policy of communicating openly and directly with the patient or his/her medical representative in the aftermath of the situation or complaint.
- We review the incident or complaint thoroughly and impartially, to assess what happened. This includes a peer review involving professionals in relevant fields. We also note any opportunities for improvement that might prevent similar situations in the future.
- If the patient has engaged legal counsel, we offer to meet with both of them to review the care and answer their questions, whether or not they have sent us a notice of intent to sue.
- If we have concluded that our care was unreasonable, we say so – and we apologize. If our care caused an injury, we work with the patient and his/her counsel to reach mutual agreement about a resolution. This doesn’t always mean a settlement, but if it does, we compensate quickly and fairly.
- If our investigation convinces us that the care was medically appropriate, we still offer to meet with the patient and his/her counsel to discuss our findings. Often, a medical staff member involved in the patient’s care will participate in this discussion. Many patients are satisfied with full explanations, and may even drop their complaint or suit. One important thing we have learned is that patients want an explanation of their care, and when they don’t get it, they frequently feel they were not treated appropriately.
- If a patient persists in a suit over care that we think was medically appropriate, or declines to participate in a dialogue with us, we will vigorously defend our staff with the finest legal team we can assemble.
- No matter what happens: We will seek to learn from the experience, educate our staff, and make changes to the systems and processes that were involved in the care that prompted the complaint. Even if our analysis convinces us that we provided medically appropriate care, the patient’s complaint teaches us that something has clouded his or her perception of our care. If we can do something to keep that from happening with another patient, we will.
Our results so far:
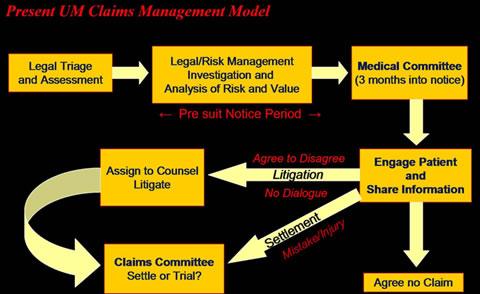
We have always worked to be open and provide full explanations to our patients. But since the year 2001, we’ve made significant changes and implemented a whole new process. Here’s what the old process looked like:

The picture is much different today. Over the past few years, we’ve been using a system that looks more like this:
One of the major features of this system is the investigation that we perform once we receive a pre-lawsuit notice, or other communication from a patient indicating that he or she has retained legal counsel and intends to file suit. We also use this approach when a major error or near-miss occurs and is reported to our Risk Management office. The process looks something like this:

This investigative step is crucial to the success of our approach. We’ve implemented many clinical improvements as a result of review of incidents, complaints and near-misses.
We’ve empowered our staff to speak up, to suggest changes, and to alert us to potential problems, including an easy-to-use secure online patient safety reporting form.
The number of claims and lawsuits has dropped dramatically. In July, 2001 we had more than 260 pre-suit claims and lawsuits pending, already an enviable number in our region. We currently have just over 100.
Our legal costs appear to be down dramatically, with the average legal expense per case down by more than 50 percent since 1997. We went to court over seven cases between Aug. 2001 and Sept. 2002, using the principle of court as the last resort. If we had lost all of them, we estimate the verdicts would have cost us more than $8 million. If we had settled all seven at the lowest pre-trial settlement demands, it would have cost about $2.5 million. We won six, and in the seventh the verdict called for a penalty of $150,000, far less than the $550,000 settlement demanded before trial. Trying all seven cost us $320,000 in legal fees. So, if you combine the settlement and the legal fees we paid, and compare it with the cost of settling all seven, we saved $2 million just in the first year of using this approach. Some of the links above contain data from later years.
The severity of our claims is rising far less rapidly than the national average. Nationally, the predicted severity of malpractice suits is rising by more than 10 percent each year. We’re also seeing an increase, but it’s about 2.6 percent each year. The slope of our claim severity graph began to change for claims arising from care in 2000, coinciding with our claims management changes in 2001 and 2002.
Opening-to-closing times for claims are dramatically shorter, down to about 10 months from more than 20 months in 2001.
Our malpractice premiums are practically level, despite increases in our clinical business. Both in terms of total expense and premium paid per adjusted hospital discharge, this goes completely against state and national trends. Because we’re self-insured, this is a true savings that helps us spend our Health System’s resources where they are needed.
We have instituted many changes to our clinical care based on lessons learned from patient complaints.
In closing... Do we think the medical malpractice system in Michigan, or in the United States, is perfect? Of course not.
We see what our colleagues in other states without reforms are going through, and we hope that change will come in a form that will provide justice for both sides. We also hope that this country will work toward ensuring that litigation is held as a last resort, and that courtroom evidence is soundly grounded in mainstream medicine and science.
But we also feel that, if there is to be any major reduction in medical malpractice claims and the financial impact they have on the medical community, there must first be an integrated approach to patient safety, quality improvement and the education of both medical staff and patients.
We hope our experience will be informative to others grappling with these same issues.